
Of all the lines Dr Rhonda Patrick delivered at Healf's HX26 conference, the one that travelled fastest around the room was about a humble fish-oil molecule. Being low in omega-3, she said, citing a large cohort study, carried a mortality risk comparable to smoking. It sounds like hyperbole. It is, in fact, a fairly literal reading of the data — and the reason omega-3 was the second item on her short list of things that move the needle on how well you age.
In Part 1 we covered vitamin D — the hormone most of us are quietly low on. Omega-3 is its natural companion in Patrick's framework: another deficiency that is widespread, largely invisible, and, crucially, measurable. Where vitamin D has its blood test, omega-3 has the Omega-3 Index — and the gap between a good number and a poor one turns out to map onto years of life.
The Claim That Sounds Like Hyperbole
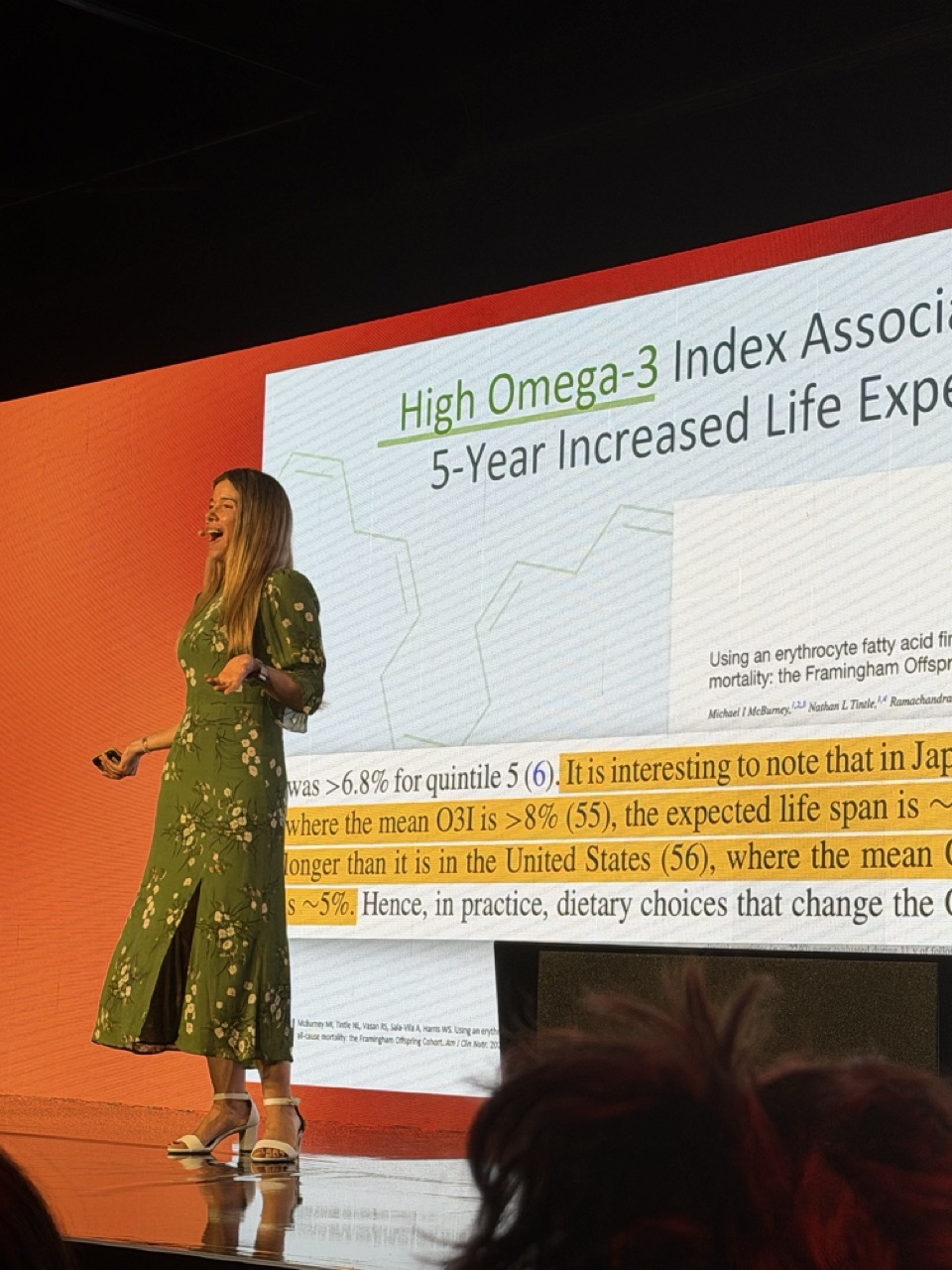
The comparison comes from work using the Omega-3 Index — a measure of how much EPA and DHA, the two marine omega-3 fats, are built into your red blood cell membranes. It is a stable, longer-term marker, reflecting roughly the past four months of intake rather than what you ate yesterday. A high index sits at 8% or above; a low one is around 4%. The average American lands near 5%; in Japan, where oily fish is a staple and heart-disease rates are famously low, the average is closer to 10%.
In a large analysis, researchers compared mortality across smoking status and omega-3 status together — and found that the two factors were of broadly similar weight. A smoker with a high omega-3 index had a life expectancy in the same region as a non-smoker with a low one. That is the sentence behind the soundbite.
Not getting enough omega-3 was, in terms of your mortality risk, essentially like smoking. That's how big a deal having a low omega-3 index is.
The headline figures she drew on are striking on their own. A high omega-3 index has been associated with around a 90% lower risk of sudden cardiac death, and, in the Framingham Offspring cohort, with roughly five extra years of life expectancy compared with a low index. These are observational associations rather than proof of cause — but the index behaves like a dial you can read, and then move.
The Heart Data, and What It Doesn't Say
Patrick was careful — more careful than the soundbite suggests — about the trial evidence, because omega-3 is a field where the studies genuinely disagree. The strongest positive result is REDUCE-IT, which gave high-risk patients 4 grams a day of a purified EPA and saw a roughly 25% reduction in major cardiovascular events. VITAL, a large prevention trial at a more typical dose, was more muted overall but showed reductions in some secondary heart-attack endpoints. A third trial, STRENGTH, was negative — which Patrick attributed in part to the particular chemical form of omega-3 it used.
Her reading of that messy literature was not "omega-3 cures heart disease." It was subtler: that the people most likely to benefit are the ones starting from a genuine deficiency, and that the blood marker — not the dose on the bottle — is what actually matters. Two people can take the same capsule and end up at very different indices.
Why It Works: Membranes and Resolution
The first thing to get right, Patrick stressed, is which omega-3 you mean. The plant form, ALA — in flax and walnuts — is only converted to the active marine forms, EPA and DHA, at very low rates in humans. When the research talks about the benefits, it is almost always EPA and DHA doing the work, and those come from oily fish or supplements, not from a spoon of ground flax.
ALA from plants barely converts. It's the EPA and DHA from fatty fish that your cells are actually using — to build membranes, and to make the molecules that switch inflammation off.
How Much — and the AFib Caveat
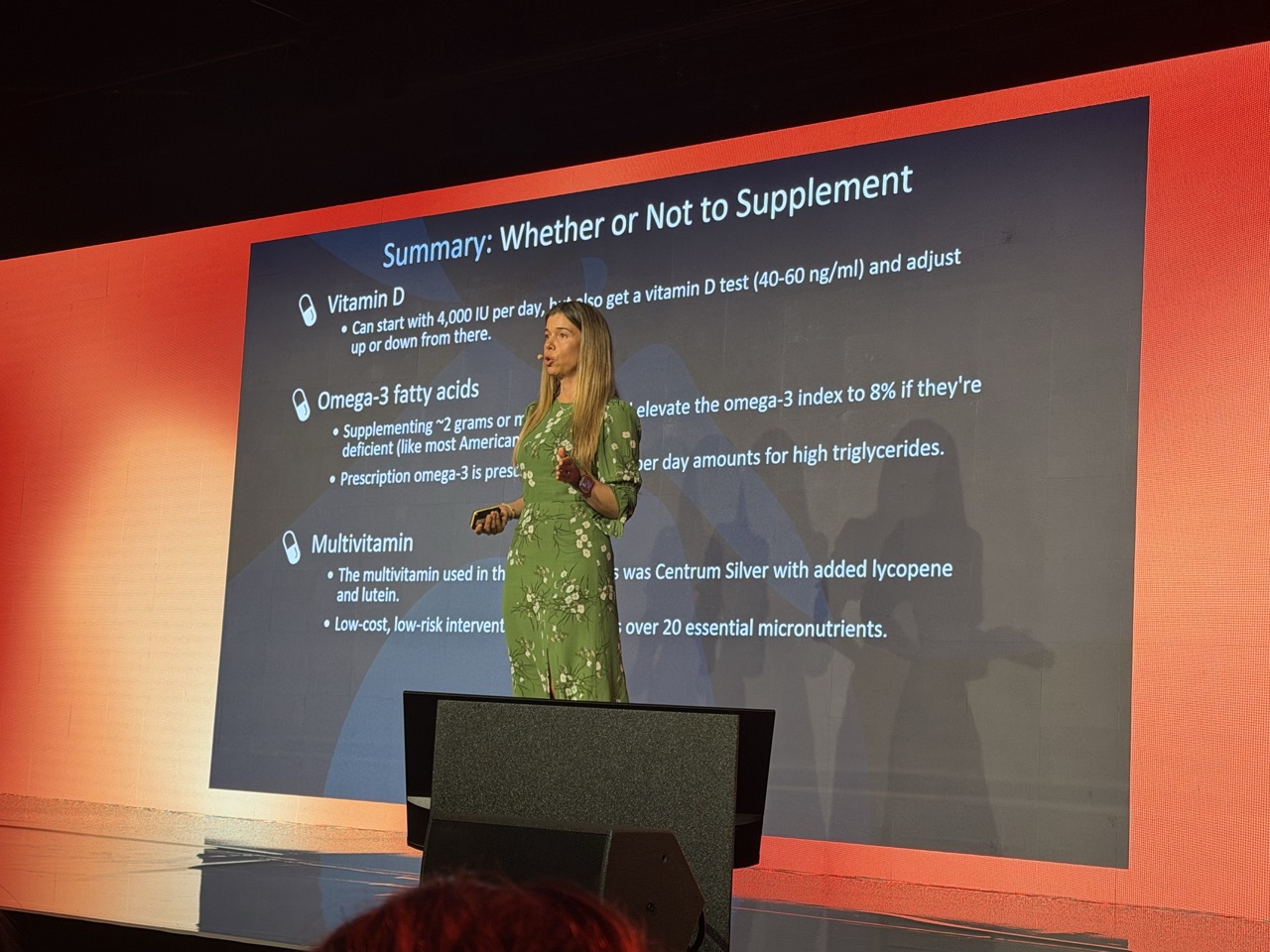
The practical target follows from the index. To lift a low reading toward the 8% range, Patrick pointed to roughly 1.6 to 2 grams of combined EPA and DHA per day for most people — achievable through two or three weekly servings of oily fish, or a supplement for those who don't eat fish. As with vitamin D, the instruction was the same: measure, adjust, and measure again a few months later.
Test your Omega-3 Index, the same way you'd check any other risk marker. Then you know whether you actually need to do anything — and whether what you're doing is working.
She was also even-handed about the one genuine safety signal, which came up in the audience questions: a small increase in the risk of atrial fibrillation seen mainly in the high-dose trials. Her framing was proportionate — the absolute increase is small, it clusters around the 4-gram doses and particular chemical forms rather than the modest amounts most people take from food or standard supplements, and it is a sensible thing to raise with your doctor if you have a personal or family history of the arrhythmia.
- 1Test your Omega-3 Index. It reflects roughly the last four months and, unlike a one-off snapshot, is a stable target to aim at. Most people have never had it measured.
- 2Eat the fish first. Two to three weekly servings of oily fish — salmon, sardines, mackerel, anchovies, herring — deliver EPA and DHA in a well-absorbed form. Plant ALA (flax, walnuts) barely converts, so it doesn't move the index much.
- 3Supplement to the target if needed. Patrick cites ~1.6–2 g/day of combined EPA+DHA to lift a low index toward 8%. Re-test after about four months to confirm you've actually got there.
- 4Flag the AFib caveat. The small atrial-fibrillation signal sits mainly with very high doses and specific forms — worth discussing with your clinician, especially with a personal or family history of AFib.
This article is educational and reports views expressed by Dr Rhonda Patrick at a public event; it is not medical advice and not a recommendation to start or change any supplement or treatment. The mortality, heart-disease and life-expectancy figures are drawn from observational cohort studies and clinical trials — they describe associations and group-level effects, not certainties for any individual, and omega-3 supplements are not a treatment for any disease. High-dose omega-3 carries a small increased risk of atrial fibrillation. Test your levels and consult a qualified clinician before starting or changing a supplement, particularly at higher doses, if you take blood-thinning medication, or if you have a history of heart-rhythm problems.
A deficiency you can
read off a dial.
The smoking comparison is designed to shock, and it does — but the more useful takeaway is quieter. Omega-3 is one of the few longevity inputs with a clean, stable blood marker attached, and the distance between a poor number and a good one is large enough to matter. You don't have to take the soundbite on faith; you can measure where you stand and decide what, if anything, to do about it.
Two pillars in, the pattern of Patrick's "80/20" is clear: cheap, measurable inputs with outsized reach. Next in the series, the one she expected the most pushback on — the much-maligned daily multivitamin, and the surprising trial data behind it.
- 01McBurney MI, Tintle NL, Vasan RS, Sala-Vila A, Harris WS. Using an erythrocyte fatty acid fingerprint to predict risk of all-cause mortality: the Framingham Offspring Cohort. American Journal of Clinical Nutrition. 2021;114(4):1447-1454.
- 02Harris WS, Tintle NL, Imamura F, et al. Blood n-3 fatty acid levels and total and cause-specific mortality from 17 prospective studies. Nature Communications. 2021;12:2329.
- 03Harris WS, von Schacky C. The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine. 2004;39(1):212-220.
- 04Bhatt DL, Steg PG, Miller M, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia (REDUCE-IT). New England Journal of Medicine. 2019;380(1):11-22.
- 05Manson JE, Cook NR, Lee I-M, et al. Marine n-3 fatty acids and prevention of cardiovascular disease and cancer (VITAL). New England Journal of Medicine. 2019;380(1):23-32.
- 06Calder PC. Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochemical Society Transactions. 2017;45(5):1105-1115.
- 07Quotations are drawn from Dr Rhonda Patrick's talk, "The Science of Slow Ageing," at Healf's HX26 conference in London, June 2026. Attributions reflect the views the speaker expressed at that event; clinical mechanisms and figures are sourced independently to the literature above. The mortality and life-expectancy figures derive from observational cohorts and describe population-level associations, not individual outcomes; trial results for cardiovascular prevention are mixed, and the atrial-fibrillation signal relates mainly to high-dose use.