
The benefits documented in Part 1 are extraordinary. But every intervention powerful enough to reshape metabolism carries risks that demand honest examination. Three concerns stand above the rest, and one of them is almost certainly the most consequential risk in modern weight-loss medicine that nobody is talking about.
GLP-1 receptor agonists are not drugs to be taken lightly, prescribed casually, or used without clinical oversight. That is not a reason to avoid them, their therapeutic potential is, in many respects, genuinely remarkable. It is a reason to understand precisely what they do to the body, where the biology creates vulnerability, and how each of those vulnerabilities can be systematically addressed. The risks covered in this article are real. They are also, with the right protocol, manageable.
Gallstone risk: the bile stasis problem
The relationship between GLP-1 therapy and gallstone formation is not a coincidence, it is a direct, mechanistic consequence of rapid weight loss. Understanding why requires a brief understanding of how cholesterol gallstones form in the first place.
When the body loses weight quickly, the liver mobilises stored cholesterol at an accelerated rate, secreting it into bile in quantities that exceed the bile's normal solubilising capacity. The result is bile that is supersaturated with cholesterol, a state in which crystals begin to precipitate out of solution. Under normal conditions, regular gallbladder contraction would flush this supersaturated bile into the small intestine before crystals can aggregate into stones. But GLP-1 receptor agonists slow gastric motility, and in doing so, they also reduce the hormonal signals that drive gallbladder contraction. Bile stasis and cholesterol supersaturation occurring simultaneously is precisely the environment in which cholesterol gallstones form.
It is worth emphasising that this is not a risk unique to GLP-1s. Gallstone formation is a well-documented consequence of any rapid weight-loss intervention, bariatric surgery carries a similarly elevated risk. Dosage and administration are determined and supervised by your prescribing clinician, who will assess individual risk factors including pre-existing gallbladder disease or a history of gallstones before beginning therapy.
Who is at highest risk
Risk is highest in patients who: lose weight very rapidly (particularly in the first four to eight weeks), have pre-existing biliary sludge, are female (women have approximately twice the gallstone incidence of men due to oestrogen effects on bile cholesterol secretion), or have a personal or family history of gallstone disease. The clinical takeaway is clear, this is a risk that warrants discussion before prescription, not discovery in the emergency department.
The thyroid cancer signal
Of the three major risks covered in this article, the thyroid signal is the one that generates the most patient anxiety, and also the one where the current evidence is most reassuring for the general population, provided the correct contraindications are observed.
In rodent carcinogenicity studies conducted as part of the regulatory approval process for semaglutide and liraglutide, GLP-1 receptor agonists were found to cause dose- and duration-dependent C-cell hyperplasia and, at high doses, medullary thyroid carcinoma. These findings triggered a black box warning that remains on all approved GLP-1 products.
After more than two decades of clinical use and post-marketing surveillance across hundreds of thousands of patients, no definitive signal for increased medullary thyroid carcinoma incidence has emerged in human data. The LEADER, SUSTAIN, and SELECT trials, collectively involving tens of thousands of patients, have not demonstrated a statistically significant increase in thyroid malignancy.
That said, surveillance is ongoing, and the absence of a definitive signal to date does not constitute proof of safety at the population level over decades of use. The appropriate response is not to dismiss the concern, it is to observe the contraindications rigorously. A personal or family history of medullary thyroid carcinoma, and Multiple Endocrine Neoplasia type 2 (MEN2) syndrome, are among the prescriber-assessed contraindications to GLP-1 therapy — suitability is determined individually by a qualified prescriber prior to initiation.
Calcitonin monitoring
Monitoring requirements for patients on long-term GLP-1 therapy are determined and supervised by your prescribing clinician.
The muscle mass crisis
Here is where the conversation becomes genuinely urgent. The gallstone risk is real but well-characterised and largely preventable. The thyroid signal is real but, in the general population without genetic predisposition, currently reassuring. The muscle mass problem is something different entirely, it is, in Dr Coetsee's framing, the risk that nobody in mainstream medicine is adequately discussing, and the one that has the greatest potential to determine the long-term health outcomes of the millions of people currently on these drugs.
The 2024 American Diabetes Association study presents a comparison of lean mass loss across a range of conditions and interventions over a 72-week period. The findings are clinically significant: lean mass losses observed with GLP-1 therapy were substantial when compared with other conditions in the analysis. The data underscores that muscle preservation is a central consideration in any GLP-1 protocol.
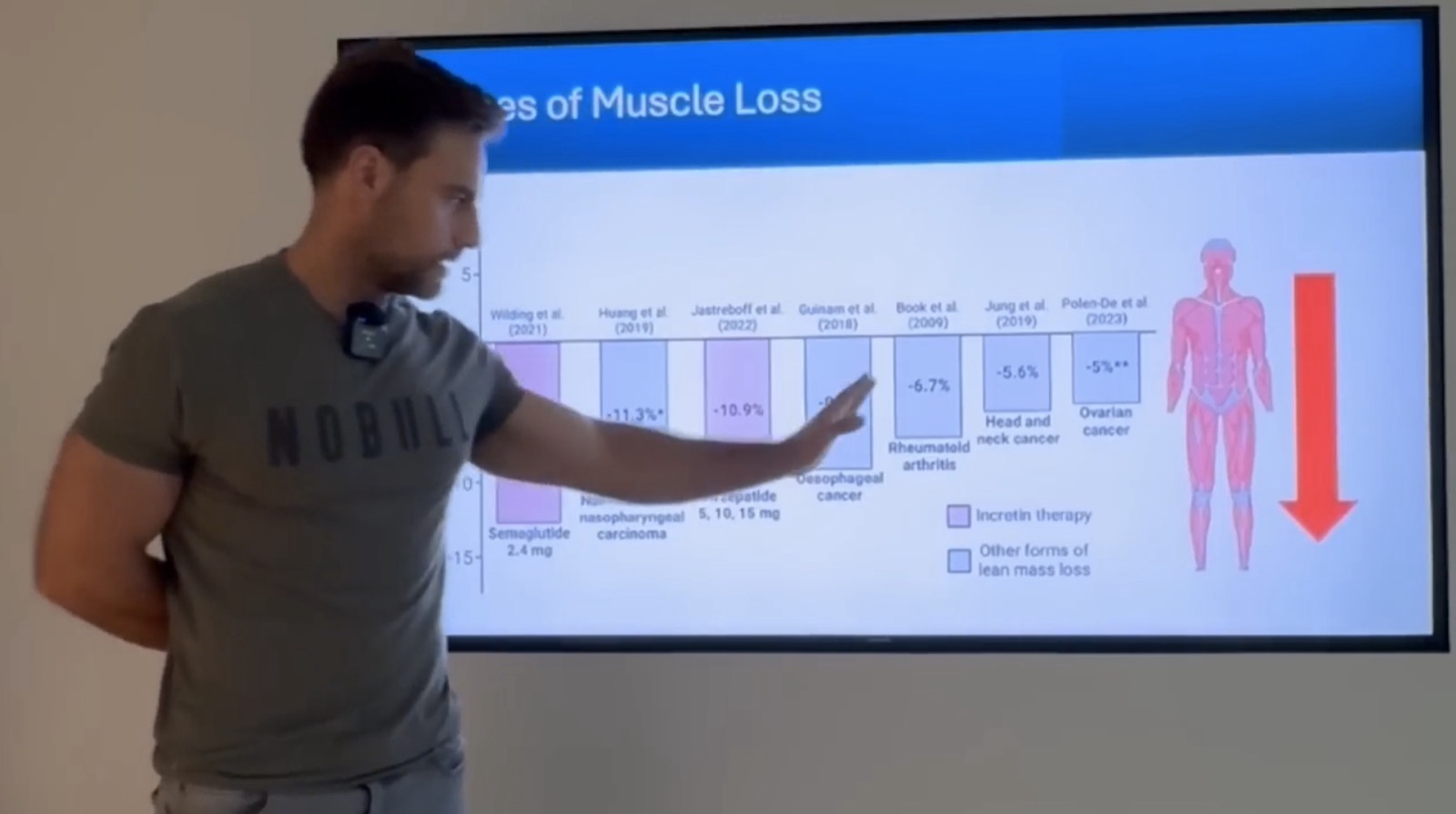
These are not edge cases or statistical artefacts. They reflect the pharmacological reality of aggressive caloric restriction combined with reduced appetite, the body, in the absence of adequate protein intake and resistance exercise stimulus, does not discriminate between fat and muscle when mobilising energy. It breaks down both, and at the doses most commonly prescribed, the lean mass losses are substantial and clinically meaningful.
Why muscle mass determines longevity
To understand why the lean mass losses documented above matter so profoundly, it is necessary to understand what muscle actually does, and it does far more than move your skeleton.
Skeletal muscle is now classified as an endocrine organ. It produces a family of signalling molecules called myokines, hormones that are secreted into the bloodstream in response to muscle contraction and that exert profound effects on multiple tissues. Irisin and IL-6, among the most studied, directly influence brain health, cardiovascular function, bone density, insulin sensitivity, and inflammatory regulation. When you lose muscle mass, you lose not just mechanical capacity, you lose a major endocrine system.
The longevity data on muscle mass is among the most consistent in geriatric medicine. Across conditions as varied as Alzheimer's disease, Parkinson's, cancer, diabetes, and acute infection, higher muscle mass is independently associated with better outcomes in multiple large observational datasets. Research consistently finds an association between greater muscle mass and lower all-cause mortality, an association that persists after adjustment for many common confounding variables (Pedersen & Febbraio, Nature Reviews Endocrinology, 2012).
This is why the muscle losses documented in GLP-1 trials are not an abstract biomarker concern. For a 55-year-old patient who loses six kilograms of lean mass over 18 months on Mounjaro and does not replace it through structured resistance training, the trajectory towards sarcopenic frailty is not a distant risk. It is an actively accelerated process.
The cognitive health dimension deserves equal attention. Myokines produced by contracting muscle, particularly brain-derived neurotrophic factor (BDNF) and irisin, cross the blood-brain barrier and have direct neuroprotective effects. Exercise-induced muscle contraction is among the most potent stimuli for BDNF production. The mechanistic link between muscle loss and cognitive decline is no longer speculative. Maintaining muscle mass is, in a very direct sense, maintaining cognitive reserve.
The body composition paradox
There is a critically important distinction that is routinely missed in discussions of GLP-1 outcomes, the difference between relative and absolute body composition changes. Dr Coetsee identifies this as the primary source of misconception in how patients and, too often, clinicians interpret the trial data.
Consider a person starting at 100 kg with a body composition of 50% muscle and 50% fat, 50 kg of muscle, 50 kg of fat. After 72 weeks on tirzepatide, they weigh 80 kg. Their body composition is now measured as 60% muscle, 40% fat. This looks extraordinary. In relative terms, the ratio has improved dramatically. But the absolute numbers tell a different story entirely.
This is the paradox: the body composition ratio displayed on a patient's DEXA scan looks better after treatment, but if absolute lean mass has declined and exercise habits have not been established, the patient's long-term metabolic and functional resilience has been compromised, not improved. The fat comes back. The muscle, without deliberate and sustained resistance training, does not.
What the trials actually show
The pivotal SURMOUNT-1 and STEP trial programmes collectively represent the most comprehensive body of evidence on tirzepatide and semaglutide outcomes in non-diabetic adults with obesity. The headline weight-loss figures, up to 22.5% of body weight at 72 weeks in SURMOUNT, are legitimate and impressive. The DEXA sub-studies, less prominently reported, tell the fuller story.
The 40-50% lean mass loss figure, meaning that roughly 40 to 50 cents in every pound of weight lost came from lean tissue rather than fat, is the central finding. For a patient who loses 20 kg, that translates to 8-10 kg of lean mass lost alongside 10-12 kg of fat. That is not a cosmetic footnote. That is a decade of age-related muscle decline compressed into 18 months.
The trial data also demonstrates that this outcome is not pharmacologically inevitable. SURMOUNT sub-group analyses comparing exercising and non-exercising participants showed dramatically different lean mass retention profiles. Participants who performed resistance training alongside tirzepatide therapy lost a far smaller proportion of lean mass and, critically, showed significantly less weight regain at 120-week follow-up, approximately 10% versus 60% in the non-exercising group.
The "skinny fat" outcome, a term Dr Coetsee uses advisedly, describes the patient who achieves impressive scale-weight reduction while retaining proportionally high visceral fat and critically reduced muscle mass. This phenotype, technically termed sarcopenic obesity, carries cardiovascular and metabolic risks that in some respects exceed those of straightforward obesity. It is, with current prescribing practice, an outcome that thousands of patients are moving towards without knowing it.
The lean mass losses documented in these trials are clinically meaningful and, with the right approach, substantially preventable. Resistance training and adequate protein intake during GLP-1 therapy change the outcome significantly.
The conclusion is not that GLP-1 receptor agonists are dangerous drugs to be avoided. It is that they are powerful tools that demand a correspondingly serious commitment to the protective protocol that must accompany them. The risks described in this article, gallstone formation, the ongoing thyroid surveillance requirement, and most critically the lean mass losses, are all addressable. Part 3 of this series lays out exactly how.
The risks are real.
They are also manageable.
if you understand them.
Gallstone risk is real but largely mitigatable through dose titration and prophylactic ursodeoxycholic acid. The thyroid signal is biologically plausible but, to date, not confirmed in human data at clinical doses, with absolute contraindications that must be respected. The muscle mass crisis is the most consequential risk in the long-term health equation, and it is the one most systematically neglected in standard care.
Part 3 of this series will lay out the exact protocol for using GLP-1 receptor agonists safely, the resistance training requirements, the protein targets, the monitoring approach, and the supplementation strategy that preserves the muscle mass on which your longevity ultimately depends. Understanding the risks is step one. Part 3 is what you do about them.
- 01Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity. New England Journal of Medicine. 2022;387(3):205-216. (SURMOUNT-1)
- 02Wilding JPH, et al. Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine. 2021;384(11):989-1002. (STEP-1)
- 03Mok J, et al. Incidence of cholelithiasis and cholecystitis in patients prescribed GLP-1 receptor agonists and their association with weight loss. JAMA Surgery. 2024;159(6):631-638.
- 04Funch D, et al. Incidence of thyroid cancer among users of GLP-1 receptor agonists in a large US insurance claims database. Diabetes, Obesity and Metabolism. 2021;23(9):2183-2193.
- 05Nauck MA, Meier JJ. GLP-1 receptor agonists and SGLT2 inhibitors: a couple at last? Lancet Diabetes & Endocrinology. 2019;7(11):822-824.
- 06American Diabetes Association. Lean and fat mass changes in adults using tirzepatide and semaglutide: analysis of 72-week DEXA data. ADA 84th Scientific Sessions. 2024. Abstract 526-P.
- 07Bhasin S, et al. Drug insight: testosterone and selective androgen receptor modulators as anabolic therapies for muscle and bone wasting. Nature Clinical Practice Endocrinology & Metabolism. 2006;2(3):146-159.
- 08Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359(9319):1761-1767.
- 09Landi F, et al. Sarcopenia as a risk factor for falls in elderly individuals: results from the ilSIRENTE study. Clinical Nutrition. 2012;31(5):652-658.
- 10Pedersen BK, Febbraio MA. Muscles, exercise and obesity: skeletal muscle as a secretory organ. Nature Reviews Endocrinology. 2012;8(8):457-465.