
GLP-1 receptor agonists, the class of injectable compounds that includes semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro), represent the most significant pharmacological advance in metabolic health in decades. But the conversation in most clinical settings, and almost everywhere in the media, stops at weight loss. That is a profound misreading of what these compounds actually do.
Understanding the mechanism is not an academic exercise. It determines how these drugs should be used, what they genuinely protect against, where their risks lie, and why the difference between semaglutide and tirzepatide is not merely a marketing distinction. The science, appraised honestly, is extraordinary, and the science, misapplied, produces predictable harm.
This is Part 1 of a three-part series. Here we cover the mechanism of action in full: what GLP-1 receptor agonists are, how they alter brain signalling and appetite, how they affect gastric motility, what they do to fat cells independent of caloric restriction, why tirzepatide's dual agonism produces superior outcomes, and what the landmark clinical trials have established. Part 2 examines the significant risks, including gallstone formation, thyroid signalling concerns, and the muscle mass problem that the weight loss data systematically obscures.
What Are GLP-1 Receptor Agonists?
GLP-1, glucagon-like peptide-1, is a peptide hormone produced naturally in the gut in response to eating. It is an incretin: a class of hormones released from the gastrointestinal tract that stimulate insulin secretion in a glucose-dependent manner, signal satiety to the brain, and modulate gastric motility. It is not a foreign compound. It is part of the body's own metabolic signalling architecture.
Exercise raises circulating GLP-1 levels by approximately four to five times above baseline, a meaningful increase, but physiologically bounded. Injectable GLP-1 receptor agonists, by contrast, raise circulating levels by roughly one thousand times the natural resting concentration. This is not an incremental augmentation of a natural process; it is a pharmacological amplification of an existing system at a fundamentally different order of magnitude.
The synthetic versions used clinically, semaglutide and tirzepatide, are structurally close to endogenous GLP-1 but engineered for durability. Natural GLP-1 has a plasma half-life of roughly two minutes, cleaved rapidly by the enzyme DPP-4. The pharmaceutical compounds are modified with DPP-4 inactivators and bound to albumin to extend half-life sufficiently for once-weekly subcutaneous injection. Administration and dosing are determined and supervised by a prescribing clinician.
GLP-1 receptors are not confined to the gut and pancreas. They are distributed across the pancreas, liver, heart, kidneys, brain, stomach, vasculature, and bone. This receptor distribution is precisely why the clinical effects of GLP-1 agonists extend so far beyond glycaemic control and body weight, and why the full profile of benefits is not intuitively predicted from the original diabetic indication.
A lot of people don't know this, but we actually produce these things naturally. When we exercise, we see GLP-1s going up in the blood, it's like four or five times raised. Whereas when we inject them, it's like a thousand times raised.
The Brain: Appetite & Food Noise
The weight loss mechanism most people ascribe to GLP-1 agonists, eating less, is accurate but incompletely characterised. The primary site of action for appetite suppression is the arcuate nucleus of the hypothalamus: a region at the base of the brain that functions as the primary integrator of metabolic signals governing both hunger and the emotional valence of eating.
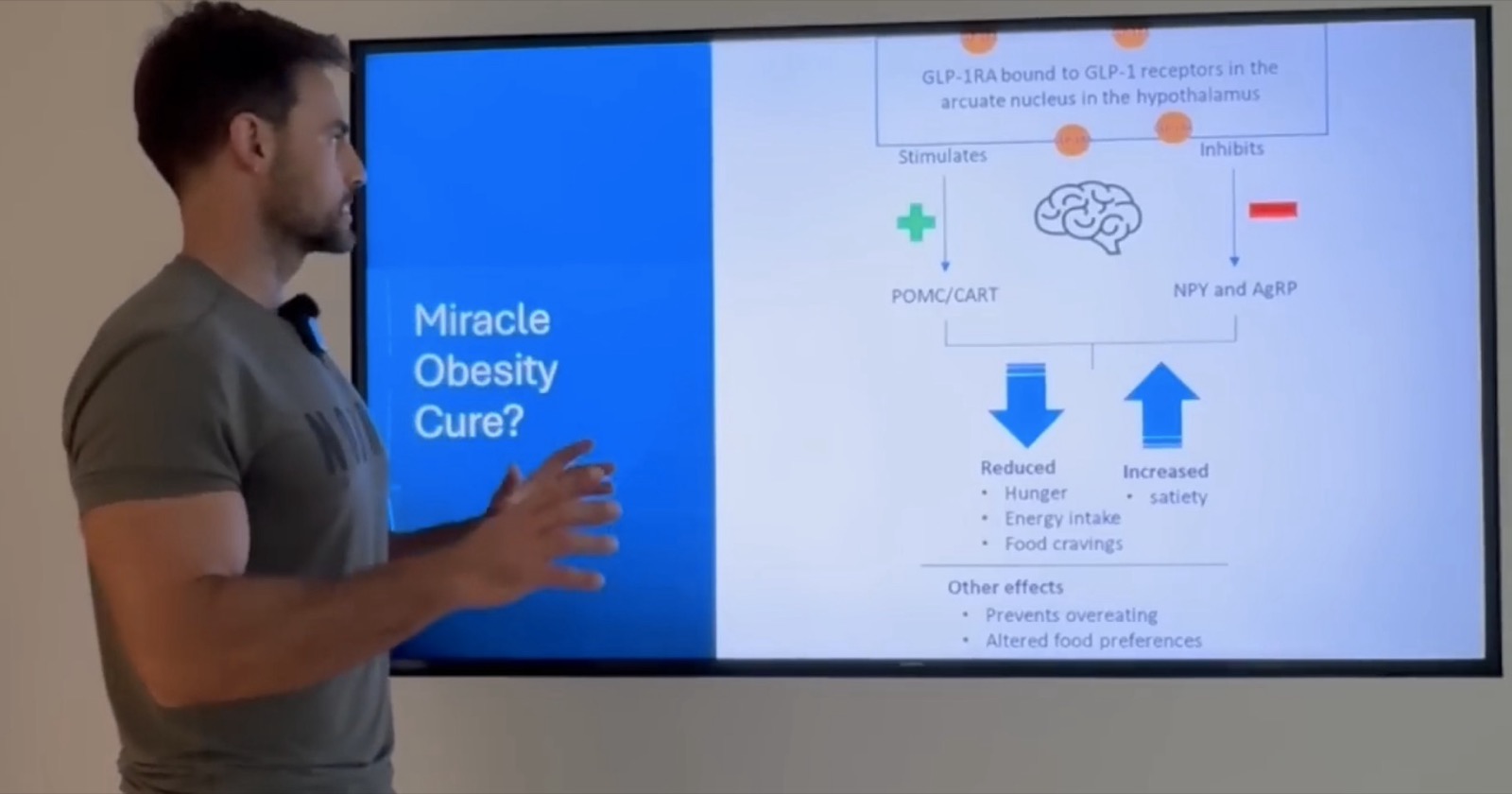
At this site, GLP-1 receptor activation produces two parallel effects. It stimulates the production of anorexigenic (appetite-suppressing) neuropeptides, the satiety signals, while simultaneously inhibiting the orexigenic pathways responsible for hunger drive, food cravings, and what has come to be described as food noise: the persistent background preoccupation with food that characterises obesity and metabolic dysregulation at a neurological level.
The consequence of this dual action is more significant than it appears on paper. Patients consistently report not merely reduced hunger but an altered relationship with food entirely. The hedonic pull of foods that previously drove compulsive eating, refined carbohydrates, alcohol, ultra-processed foods, is substantially diminished. Food preferences themselves appear to shift, with patients gravitating toward protein and whole foods not through discipline but through genuine change in appetite architecture. The tediousness of dieting, for many patients, simply disappears.
This is a neurological effect, not a motivational one. The arcuate nucleus sits at the interface of metabolic and limbic signalling, it governs not just hunger but the emotional and reward-mediated components of eating behaviour. GLP-1 receptor activation modulates both simultaneously. Reduced hunger, better energy stability, elimination of food cravings, and a shift in food preference are the mechanistic consequences, each documented in the clinical literature and reported across patient populations.
Gastric Emptying & Digestion
The second major mechanism contributing to caloric restriction under GLP-1 therapy is the direct effect on gastric motility. GLP-1 receptor activation in the stomach slows gastric emptying, the rate at which food passes from the stomach into the small intestine. Food remains in the stomach for a substantially longer period following a meal, producing mechanical satiety: a physical sense of fullness that persists well beyond what the caloric content of the meal would otherwise sustain.
This slowing of gastric transit is also the proximate cause of the most commonly reported gastrointestinal side effects, nausea, early satiety, and, at higher doses, vomiting. These effects are dose-dependent and typically resolve within the first several weeks of treatment as physiological tolerance to the gastric motility changes develops. The clinical implication is that dose titration, initiating at low doses and escalating gradually, is not merely a convention but a mechanistic necessity for tolerability.
The gastric emptying effect also has secondary metabolic consequences. Delayed nutrient absorption flattens postprandial glucose excursions, contributing to improved glycaemic control even independently of pancreatic insulin secretion effects. This is one of several mechanisms through which GLP-1 agonists improve metabolic markers through pathways that do not depend on weight loss itself.
This is the primary driver of caloric deficit in GLP-1 therapy, not metabolic rate change, not malabsorption, not surgical anatomy alteration. The caloric reduction is neurologically mediated, which is why it persists without the psychological burden of conventional dietary restriction.
Nausea experienced on GLP-1 therapy is a direct consequence of this mechanism, not a systemic toxicity. Its dose-dependence and resolution with titration confirm this.
Direct Fat Cell Effects
Perhaps the most underappreciated dimension of GLP-1 receptor agonist therapy is its direct action on adipose tissue, effects that are demonstrably independent of caloric restriction and weight loss. The fat cell is not a passive energy storage depot. It is now classified as an endocrine organ: it secretes cytokines and adipokines that mediate systemic inflammation, modulate insulin sensitivity, and influence cardiovascular risk. In metabolic disease, this endocrine function becomes profoundly dysfunctional.
GLP-1 and GIP receptors are expressed on adipocytes directly. When activated, particularly through tirzepatide's dual agonism, these receptors initiate a programme of metabolic rehabilitation in fat tissue that is independent of the weight lost. The fat cell becomes, in a measurable sense, healthier: it produces fewer pro-inflammatory cytokines, responds more appropriately to insulin, and participates more productively in normal metabolic signalling.
Brown versus white fat differentiation
Adipose tissue is not homogeneous. White adipose tissue stores energy; brown adipose tissue dissipates it as heat through uncoupled mitochondrial respiration. Brown fat is metabolically active, thermogenic, and associated with improved insulin sensitivity. Obese individuals have a reduced proportion of brown adipose tissue and a correspondingly impaired thermogenic capacity. GLP-1 receptor activation on adipocytes has been shown to promote browning, the conversion of white adipocytes toward a brown or beige phenotype, increasing thermogenic activity and improving the metabolic quality of the fat depot.
Visceral fat reduction and inflammation
The distribution of fat loss under GLP-1 therapy is not uniform. Visceral adipose tissue, the fat that accumulates around abdominal organs and is most strongly associated with cardiovascular and metabolic risk, is reduced preferentially compared to subcutaneous fat. As one study in the literature directly states: "Visceral fat is influenced to a greater extent than subcutaneous fat, inferring that GLP-1 therapy gives benefits that caloric restriction alone cannot."
Dysfunctional adipose tissue in metabolic disease produces a pro-inflammatory milieu: elevated TNF-α, IL-6, and other cytokines that drive systemic inflammation, impair insulin signalling across tissues, and directly contribute to atherosclerotic progression. GLP-1 agonists suppress these cytokine pathways at the level of the fat cell itself, decreasing adipose inflammation, reducing fibrosis, restoring normal adipokine profiles, and blocking the migration of adiposity from subcutaneous to visceral depots.
The metabolic consequence is striking: patients on GLP-1 therapy show improvements in insulin sensitivity and inflammatory markers even in the absence of significant weight loss. The drug is not simply making patients thinner, it is making their fat cells less harmful to their metabolic health, independent of how much fat they retain.
GIP: Why Mounjaro Targets Two Receptors
Semaglutide (Ozempic, Wegovy) is a selective GLP-1 receptor agonist. Tirzepatide (Mounjaro) is a dual agonist: it activates both the GLP-1 receptor and the GIP receptor, the receptor for glucose-dependent insulinotropic polypeptide, the other major incretin hormone. This dual mechanism is not incidental. It is the structural reason tirzepatide consistently produces superior weight loss and metabolic outcomes compared to semaglutide in head-to-head comparison.
GIP receptors are expressed at high density on adipocytes. When tirzepatide activates the GIP receptor on fat cells, in the context of meal-stimulated insulin secretion, it initiates a distinct programme of adipocyte metabolic rehabilitation. Glucose uptake into fat cells improves. Free fatty acid uptake and oxidative utilisation improve. Insulin resistance at the adipocyte level is substantially reduced. The fat cell becomes more metabolically competent, more capable of participating appropriately in energy homeostasis, rather than simply a dysfunctional inflammatory organ.
The GLP-1 and GIP signalling pathways in adipose tissue are complementary rather than redundant. GLP-1 receptor activation primarily drives the central appetite and gastric motility effects, with secondary adipose effects. GIP receptor activation works predominantly at the adipocyte level to improve the metabolic quality of fat tissue directly. The combination produces superior outcomes in insulin sensitivity, body composition, and long-term metabolic health than either pathway alone.
This is also why patients on tirzepatide, even those who achieve equivalent caloric restriction to patients on semaglutide, tend to show greater improvements in metabolic markers: the GIP component is generating metabolic benefit at the tissue level through pathways that GLP-1 alone does not fully engage.
The net result is that patients on tirzepatide remain metabolically healthy at a cellular level even before significant weight is lost, and achieve superior weight loss outcomes once caloric restriction is established. In the SURMOUNT-1 trial, tirzepatide at the 15mg dose produced a mean body weight reduction of 22.5% at 72 weeks, compared to approximately 15% with semaglutide 2.4mg in the STEP-1 trial.
The Landmark Trial Data
The clinical trial programme for GLP-1 receptor agonists is now among the most extensive in metabolic pharmacology. Across the STEP programme (semaglutide), the SURMOUNT programme (tirzepatide), and the SELECT cardiovascular outcomes trial, the evidence base has expanded well beyond the original glycaemic indication into cardiovascular, hepatic, and renal disease prevention, in populations without diabetes.
The SELECT Trial, cardiovascular outcomes in non-diabetic patients
The SELECT trial enrolled 17,604 overweight or obese adults with established cardiovascular disease but without diabetes, randomising them to weekly semaglutide 2.4mg or placebo. At a mean follow-up of 39.8 months, semaglutide produced a 20% reduction in the composite of cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke, major adverse cardiovascular events, compared to placebo. This was the first large-scale trial to demonstrate primary cardiovascular event reduction with a GLP-1 agonist in a non-diabetic population.
The trial also found a 13% reduction in cardiovascular death alone, a 10% reduction in myocardial infarction, and a 35% reduction in coronary revascularisation procedures. The magnitude of cardiovascular benefit was comparable to, and in some analyses exceeded, that seen with high-intensity statin therapy, a comparison that carries significant clinical implications for the treatment of obese patients with cardiovascular risk.
SURMOUNT-1, tirzepatide weight loss outcomes
The SURMOUNT-1 trial enrolled 2,539 adults with obesity or overweight without diabetes, randomising them to tirzepatide at 5mg, 10mg, or 15mg weekly, or placebo. At 72 weeks, mean weight reductions were 15.0%, 19.5%, and 20.9% respectively from baseline, with 22.5% achieved in the 15mg group among those who completed treatment per protocol. The effect size substantially exceeded what had been observed with semaglutide monotherapy and approached the weight loss seen with bariatric surgery in some analyses, a comparison previously considered pharmacologically unreachable.
STEP trials, semaglutide weight loss programme
The STEP programme (Semaglutide Treatment Effect in People with Obesity) across four main trials established semaglutide 2.4mg as producing approximately 14.9% body weight loss at 68 weeks in adults without diabetes (STEP-1), with augmented effects when combined with intensive behavioural intervention (STEP-3) and demonstrated weight regain upon discontinuation in STEP-4, an important finding regarding the chronic disease model of obesity treatment that informs current clinical guidance on long-term use.
Liver disease: an area of active GLP-1 research
Metabolic-associated steatohepatitis (MASH, formerly NASH), the inflammatory phase of non-alcoholic fatty liver disease, represents one of the most significant unmet medical needs in hepatology. In clinical trials of these prescription medicines, researchers have reported improvements in liver disease markers. (These are findings about prescription medicines, not about any BODY HLTH product.)
The mechanism operates through multiple pathways: improved hepatic insulin sensitivity reduces de novo lipogenesis and VLDL production; decreased systemic inflammation reduces hepatic inflammatory infiltrate; direct hepatocyte GLP-1 receptor signalling reduces gluconeogenesis. The combined effect is regression of steatosis, fibrosis resolution, and in some cases reversal of the histological features of advanced liver disease, a finding with no equivalent in conventional pharmacotherapy.
Beyond Weight Loss
The breadth of organ-level benefit from GLP-1 receptor agonism extends beyond any single disease model. This is not coincidental, it reflects the fundamental role of chronic inflammation and insulin resistance in the pathogenesis of virtually every age-related non-communicable disease. By targeting these upstream pathways, GLP-1 agonists produce benefits that cascade across organ systems simultaneously.
Cardiovascular protection, multiple mechanisms
Beyond the SELECT trial's outcomes data, the mechanistic basis for cardiovascular protection is well characterised. GLP-1 receptor activation on vascular smooth muscle and endothelium reduces sympathetic tone, promotes vasodilation, stabilises atherosclerotic plaques by suppressing the pro-inflammatory pathways that drive plaque rupture, reduces LDL-cholesterol and triglyceride levels, and lowers blood pressure through a three-pathway mechanism: central reduction of sympathetic nervous system activity, direct vascular smooth muscle relaxation, and renal sodium regulation. These effects compound: patients on semaglutide show reductions in C-reactive protein, improved heart failure biomarkers, and reduction of pericardial fat, the adipose depot most tightly associated with cardiac risk.
Kidney protection
GLP-1 receptors in the renal tubules regulate sodium reabsorption. By modulating tubular sodium handling, GLP-1 agonists reduce the excessive sodium retention that contributes to hypertension and chronic kidney disease progression in metabolic syndrome. Emerging data from dedicated renal outcomes trials demonstrate reductions in proteinuria, slower eGFR decline, and reduction in major kidney disease events, consistent with the mechanism and now increasingly cited in nephrology guidelines for the management of diabetic kidney disease.
Neuroprotection and cognitive health
GLP-1 receptors in the central nervous system are expressed on both neurons and microglia, the brain's resident immune cells. In the presence of neurological insult (infection, injury, amyloid accumulation), microglial activation normally drives a progressive pro-inflammatory cascade that accelerates neurodegeneration in conditions such as Alzheimer's and Parkinson's disease. GLP-1 agonists block multiple steps in this cascade, reducing microglial hyperactivation, decreasing pro-inflammatory cytokine production, and protecting neurons from apoptosis.
Researchers are also investigating these medicines in other conditions; this is early clinical research, not established use. Researchers are studying the broader effects of this drug class in neurological contexts; these are areas of ongoing investigation.
The picture that emerges is of a compound class that, at appropriate doses, acts as a systems-level anti-inflammatory and metabolic-rehabilitative agent. The weight loss is real and clinically significant. But it is the downstream consequence of an upstream mechanism, and that mechanism produces benefits that extend far beyond what the scales record.
These compounds represent a genuine
paradigm shift in metabolic medicine.
not merely a weight loss tool.
GLP-1 receptor agonists, understood at the level of their mechanisms, are not primarily weight loss drugs. They are metabolic rehabilitators: compounds that act on the hypothalamus, gastric motility, adipocytes, vasculature, liver, kidneys, and brain simultaneously to restore the conditions of metabolic health. The weight loss that follows is a consequence of this restored signalling, not the mechanism itself.
But understanding the mechanism is only half the story. The same potency that makes these compounds so effective is also the source of risks that are frequently minimised or omitted from public discourse, gallstone formation, thyroid signalling concerns, and a lean mass loss profile that the body weight data systemically obscures. Part 2 examines those risks with the same rigour applied here to the benefits.
- 01Lincoff AM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. New England Journal of Medicine. 2023;389(24):2221-2232. [SELECT Trial]
- 02Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity. New England Journal of Medicine. 2022;387(3):205-216. [SURMOUNT-1]
- 03Wilding JPH, et al. Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine. 2021;384(11):989-1002. [STEP-1]
- 04Perkovic V, et al. Semaglutide and kidney outcomes in type 2 diabetes and chronic kidney disease. New England Journal of Medicine. 2024;391(2):109-121. [FLOW Trial]
- 05Newsome PN, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. New England Journal of Medicine. 2021;384(12):1113-1124. [NASH/MASH]
- 06Müller TD, et al. Glucagon-like peptide 1 (GLP-1). Molecular Metabolism. 2019;30:72-130.
- 07Nauck MA, et al. Reduced incretin effect in type 2 (non-insulin-dependent) diabetes. Diabetologia. 1986;29(1):46-52.
- 08Kosiborod MN, et al. Semaglutide in patients with heart failure with preserved ejection fraction and obesity. New England Journal of Medicine. 2023;389(12):1069-1084. [STEP-HFpEF]
- 09Svendsen B, et al. Adipose tissue: a novel target of the incretin axis? Frontiers in Endocrinology. 2020;11:572070.
- 10Holst JJ. The physiology of glucagon-like peptide 1. Physiological Reviews. 2007;87(4):1409-1439.